Clinical Context: Why Adenoma Detection Rate Matters and Where Colonoscopy Falls Short
Colorectal cancer remains one of the leading causes of cancer-related death worldwide, with approximately 1.9 million new cases and 930,000 deaths recorded annually by GLOBOCAN estimates. Colonoscopy is the primary tool for both detection and prevention — but its protective effect depends heavily on whether the endoscopist actually finds the adenomas that are there.
Adenoma detection rate (ADR) — the proportion of screening colonoscopies in which at least one adenoma is identified — is the dominant quality metric in endoscopy practice. The clinical stakes are high: each 1% increase in ADR is associated with approximately a 3% reduction in the risk of interval colorectal cancer, the cancers that develop between scheduled colonoscopies. Endoscopists with lower ADRs leave more adenomas behind.
The miss rate problem is substantial. Studies using back-to-back tandem colonoscopy designs estimate that 20–26% of adenomas are not detected on a standard examination. The lesions most likely to be missed are not the large, protruding, already-conspicuous ones — they are the small, flat, and serrated lesions that blend into the mucosal background. Sessile serrated lesions (SSLs) are a particular concern: they are precursors to a distinct pathway of colorectal cancer, they are disproportionately located in the right colon where visualization is harder, and they are consistently underdetected even by experienced endoscopists.
Computer-aided detection (CADe) systems were developed to address this gap by providing real-time visual and auditory alerts during the withdrawal phase of colonoscopy. Across multiple platforms, the pooled RCT evidence shows meaningful ADR gains — the broader mixed-platform evidence base, covered in depth in the companion article on AI-assisted colonoscopy polyp detection RCT evidence, reports a 20% relative ADR increase across 28 RCTs. The question this digest addresses is narrower and more clinically actionable: what does the evidence show specifically for GI Genius, the first CADe device cleared by the US FDA, when analyzed in isolation from other platforms?
GI Genius: Device Background and FDA Regulatory Status
GI Genius (Medtronic, developed in collaboration with Cosmo Pharmaceuticals) was the first CADe system to receive US FDA authorization via the de novo pathway, granted in 2021. De novo authorization establishes a new device classification for novel low-to-moderate risk devices without a legally marketed predicate — a regulatory pathway distinct from the 510(k) substantial equivalence route used by many subsequent CADe systems.
The system integrates with standard endoscopy hardware and software stacks. During the colonoscope withdrawal phase, the AI module processes the live video feed in real time, overlaying a green rectangular bounding box on areas of the mucosal surface it identifies as potentially containing a polyp and generating an audio alert. The device is designed to function as a second-look tool — drawing the endoscopist's attention to regions they might otherwise pass over.
- Intended use: real-time detection assistance during colonoscope withdrawal; not intended to characterize lesions for biopsy decisions or replace endoscopist clinical judgment.
- Regulatory pathway: FDA de novo clearance (2021), establishing a new device classification for AI-based CADe systems.
- Mechanism: convolutional neural network processing live endoscopy video; outputs a bounding-box overlay and audio alert when a potential polyp is detected.
- Integration: compatible with standard endoscopy imaging stacks; does not require replacement of existing hardware.
Study Design: The First GI Genius-Specific Systematic Review and Meta-Analysis
The anchor study for this digest is Sattar et al. (Cureus, October 2025; PMC12616575; PMID 41246784) — the first PRISMA-aligned systematic review and meta-analysis restricted exclusively to randomized controlled trials of the GI Genius system. Prior meta-analyses of CADe colonoscopy have pooled data across multiple platforms, making it impossible to isolate device-specific performance. This study addresses that gap directly.
The search covered PubMed, Embase, and CENTRAL through August 25, 2025. After screening 4,313 records, 7 RCTs met inclusion criteria, enrolling a total of 9,639 patients. Risk of bias was assessed using the RoB 2 tool. GRADE certainty of evidence was applied per outcome. Pooled effect sizes were calculated using random-effects models in RevMan 5.4.1.
| Trial | Country / Setting | N | Population Note |
|---|---|---|---|
| COLO-DETECT (Seager et al.) | UK (12 NHS hospitals) | 2,032 | Routine colonoscopy; Medtronic-funded; multiple authors with Medtronic COI |
| COLO-GENIUS (Karsenti et al.) | France (single non-academic centre) | 2,015 | Routine colonoscopy; no industry funding declared |
| Mangas-Sanjuan et al. | Spain | 3,213 | Largest single trial in the meta-analysis |
| Repici et al. (2020) | Italy | 685 | Early GI Genius RCT; academic centre |
| Wallace et al. (2022) | Italy / UK / US (multinational) | 230 | Smaller multinational trial |
| Thiruvengadam et al. (2024) | US (single centre) | 1,100 | Only US-based trial in the meta-analysis |
| TIMELY / Ortiz et al. | Spain / Italy / Germany / Belgium | 430 | Lynch syndrome population; multinational European |
Primary Outcome — Adenoma Detection Rate: A Statistically Significant but Heterogeneous Gain
Across all 7 RCTs, GI Genius-assisted colonoscopy produced a statistically significant increase in adenoma detection rate compared with standard colonoscopy: relative risk 1.12 (95% CI 1.03–1.22, p=0.01). In clinical terms, this translates to approximately one additional adenoma detected for every 8–10 patients examined — a meaningful yield in a screening context where each missed adenoma represents a potential future cancer.
However, the GRADE certainty for this outcome was rated moderate, not high. The primary reason for downgrading was substantial statistical heterogeneity: I²=64%. This level of heterogeneity indicates that the true effect of GI Genius on ADR varies meaningfully across the included trials — likely reflecting differences in baseline endoscopist ADR, patient populations, bowel preparation quality, and system activation protocols. GRADE moderate certainty means that further well-designed trials could change the pooled estimate, and clinicians should not treat the 12% figure as a fixed, universally applicable effect size.
Secondary Outcomes: PDR, SSLDR, and Adenomas Per Colonoscopy
The secondary outcomes in the Sattar et al. meta-analysis present a more consistent and, in several cases, more certain picture than the primary ADR finding. The most clinically differentiated result is the sessile serrated lesion detection rate (SSLDR), which showed a 27% relative increase with high GRADE certainty — the strongest and most reliable finding in the entire analysis.

| Outcome | Effect Size | 95% CI | I² | Trials / N | GRADE Certainty |
|---|---|---|---|---|---|
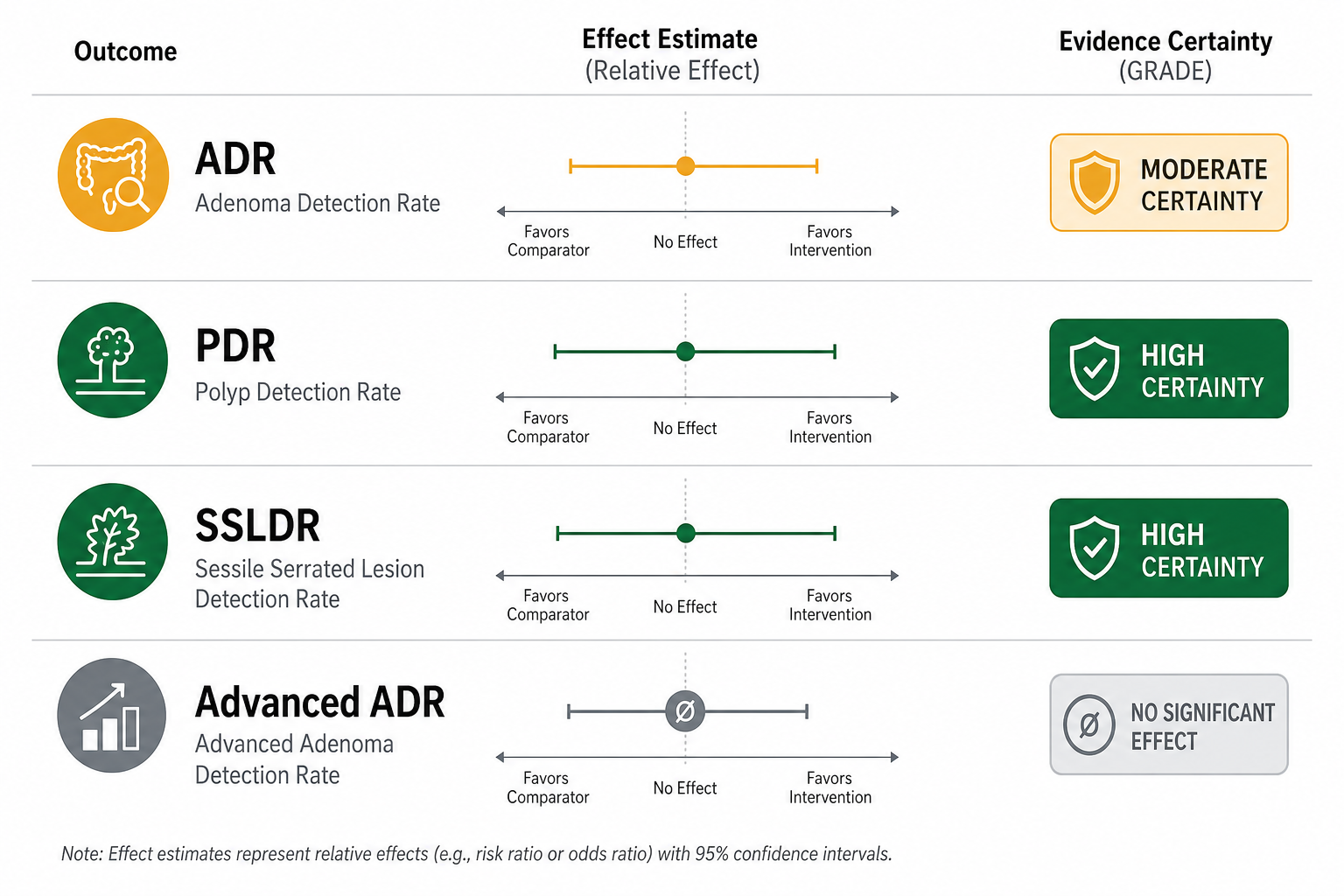
| ADR (Adenoma Detection Rate) | RR 1.12 | 1.03–1.22 | 64% | 7 RCTs / 9,639 | Moderate (downgraded: inconsistency) |
| PDR (Polyp Detection Rate) | RR 1.05 | 1.01–1.10 | 0% | 2 RCTs / 5,225 | High |
| SSLDR (Sessile Serrated Lesion Detection Rate) | RR 1.27 | 1.11–1.47 | 11% | 4 RCTs / 7,013 | High |
| APC / MAP (Adenomas Per Colonoscopy / Mean Adenomas Per Patient) | SMD 0.15 | 0.09–0.20 | 29% | Multiple RCTs | High |
| PPC / MP (Polyps Per Colonoscopy / Mean Polyps) | SMD 0.10 | 0.05–0.15 | 0% | Multiple RCTs | High |
| Advanced ADR | RR 1.01 | 0.90–1.13 | 6% | Multiple RCTs | Moderate (downgraded: imprecision) |
The SSLDR finding deserves particular attention for two reasons. First, at high GRADE certainty and I²=11%, it is the most statistically consistent result in the analysis — the effect is present across contributing trials with minimal between-study variation. Second, this finding stands in contrast to the broader mixed-platform meta-analysis by Makar et al. (GIE 2024), which did not find a statistically significant SSLDR benefit in its overall CADe analysis (RR 1.10, not significant) and did not confirm a significant SSLDR effect in its GI Genius-specific subgroup. The device-specific meta-analysis, drawing on more GI Genius trials than any prior subgroup analysis, provides stronger and more direct evidence for this outcome than has previously been available.
PDR — the proportion of procedures detecting at least one polyp of any histology — increased by 5% (RR 1.05, I²=0%, high certainty) across two large trials totaling 5,225 patients. The near-zero heterogeneity and high GRADE rating make this a reliable estimate, though the absolute magnitude is modest. The APC and PPC metrics, which measure how many adenomas or polyps are found per procedure rather than simply whether any are found, both showed consistent high-certainty improvements, confirming that GI Genius increases yield across multiple counting approaches, not just binary detection thresholds.
The Critical Null Finding: Advanced Adenoma Detection Rate
The most clinically important finding in this meta-analysis is not what GI Genius improves — it is what it does not. Advanced adenoma detection rate showed no statistically significant improvement: RR 1.01 (95% CI 0.90–1.13, p=0.85, I²=6%). GRADE certainty was rated moderate, downgraded for imprecision.
Advanced adenomas — defined as adenomas ≥10 mm, with high-grade dysplasia, or with villous histology — are the lesions most directly associated with near-term colorectal cancer risk. The null finding here has a coherent clinical explanation: advanced adenomas are already large and conspicuous enough that experienced endoscopists detect them at similar rates with or without AI assistance. The AI's marginal contribution concentrates on the subtle, small (1–5 mm), flat, and serrated lesions that are genuinely difficult to see against the mucosal background — precisely the lesion types where the SSLDR and small-polyp ADR gains are observed.
This null finding does not undermine the case for GI Genius; it clarifies it. The device's clinical value lies in a specific and meaningful niche: reducing the miss rate for subtle lesions — particularly sessile serrated lesions — that experienced endoscopists would otherwise overlook. That is a real and important benefit. It is simply not the benefit of catching the lesions that were already being caught.
Risk of Bias and Methodological Considerations
The RoB 2 assessment rated 6 of the 7 included RCTs as either low risk or raising some concerns. One trial was rated high risk, specifically in domain 4 (outcome measurement), meaning there were concerns about how adenoma detection was ascertained or recorded in that trial. The authors do not identify which trial received the high-risk rating by name in the publicly available summary, but the overall bias profile across the included trials is reasonably favorable.
- Blinding of endoscopists is structurally impossible in CADe trials — endoscopists can see the bounding-box overlay and hear the audio alert. This is a systemic limitation across all colonoscopy AI RCTs, not a flaw specific to any single GI Genius trial. It introduces the possibility of performance bias in both directions: endoscopists in the intervention arm may examine more carefully, while those in the control arm may examine less carefully if they know AI is available in the other arm.
- The most common RoB 2 concern across trials was domain 2 (blinding of participants and personnel), consistent with the above structural limitation.
- The COLO-DETECT trial — the largest single trial in the meta-analysis (n=2,032, 12 NHS hospitals in England) — was funded by Medtronic, and several lead authors received Medtronic grant funding or honoraria. This is a material conflict of interest that readers should note when interpreting that trial's individual results, even though its inclusion in the pooled meta-analysis dilutes its individual influence.
- The Sattar et al. meta-analysis itself declared no industry funding and no author financial conflicts — a favorable COI profile relative to many device-specific studies in this field.
Limitations: What the Evidence Cannot Yet Answer
- Moderate ADR heterogeneity (I²=64%) with unexplained sources. The meta-analysis does not fully account for why the ADR effect varies so substantially across trials. Likely contributors include differences in baseline endoscopist ADR, patient bowel preparation quality, colonoscopy indication (screening vs. surveillance vs. diagnostic), and system activation protocols — but these were not formally analyzed as heterogeneity moderators.
- Fewer than 10 trials per outcome, precluding formal publication bias assessment via funnel plots. The direction of benefit is consistent across trials, but small-study effects — where smaller trials tend to report larger effect sizes — cannot be excluded.
- Predominantly European trial populations. Six of the seven included RCTs were conducted in the UK, France, Spain, Italy, Germany, or Belgium. The one US trial (Thiruvengadam 2024) was a single-center study. The TIMELY trial enrolled a Lynch syndrome population, which has distinct adenoma biology and is not representative of general screening colonoscopy. Direct generalizability to diverse US endoscopy practice settings — particularly community practices, federally qualified health centers, or lower-resource settings — is uncertain.
- No long-term endpoints. None of the included trials measured colorectal cancer incidence or cancer-specific mortality. The clinical assumption is that improved adenoma detection translates to reduced cancer incidence, but this has not been directly tested for GI Genius in any of the included trials.
- Real-world gains are likely smaller than RCT estimates. In RCTs, endoscopists know they are being observed and that the AI system is active — conditions that may not replicate in routine practice. Variable system activation rates, inconsistent alert response behavior, and endoscopist fatigue in high-volume units may all attenuate the effect observed under trial conditions.
Real-World Implementation: What US Practice Data Add
A retrospective US study by Kim et al. (Clinical Endoscopy, 2025) at Weill Cornell Medical Center provides important context for interpreting the pooled RCT findings in a high-volume, high-baseline-ADR academic setting. The study covered 798 colonoscopies performed by 16 endoscopists, all of whom had baseline ADRs of 35% or higher — well above the national quality benchmark.
The key finding: GI Genius alone produced no statistically significant improvement in overall ADR, adenomas per colonoscopy, SSLDR, or advanced ADR in this high-performing cohort. Statistically significant improvements in 1–5 mm ADR (36.3% to 52.1%), 1–5 mm SSLDR (9.6% to 17.1%), right-sided ADR (30.8% to 42.7%), and right-sided SSLDR (12.3% to 24.8%) were observed only when GI Genius was combined with EndoCuff — a physical cap device that improves mucosal visualization by flattening haustral folds.
This pattern — AI assistance producing measurable gains primarily in combination with other quality-improvement tools, and showing attenuated effects in high-ADR endoscopists — is consistent with a broader pattern observed across FDA-cleared AI medical devices. The gap between RCT performance and real-world deployment outcomes has been documented in other specialties as well; the evidence on AI for diabetic retinopathy screening illustrates the same dynamic: controlled trial performance does not automatically transfer to heterogeneous real-world deployment environments.
One additional real-world trade-off deserves acknowledgment. The broader 28-RCT mixed-platform meta-analysis (Makar et al., GIE 2024) found a 39% increase in non-neoplastic resection associated with CADe use — meaning that AI detection alerts lead to a meaningful increase in the removal of lesions that turn out not to be adenomas. This is not a finding specific to Sattar et al., and the GI Genius-specific meta-analysis does not report it as a primary outcome, but it is a systemic trade-off of CADe adoption that technology committees should factor into their analysis of procedural volume, pathology costs, and patient risk from unnecessary resection.
Clinical Relevance and Evidence Summary
The Sattar et al. (2025) meta-analysis is the most methodologically rigorous device-specific evidence available for GI Genius as of mid-2026. It isolates GI Genius performance from the mixed-platform CADe literature, applies GRADE appraisal per outcome, and does so without industry funding or author financial conflicts. For gastroenterologists and hospital technology committees evaluating the device, the key evidence points are as follows.

- What the evidence supports: Routine activation of GI Genius for standard colonoscopy is associated with a statistically significant 12% relative increase in ADR (GRADE moderate) and a 27% increase in SSLDR (GRADE high). The SSLDR finding is the strongest and most consistent result in the analysis — it carries high certainty, low heterogeneity, and is based on 4 RCTs covering over 7,000 patients.
- What the evidence does not support: GI Genius does not significantly improve detection of advanced adenomas (RR 1.01, p=0.85, GRADE moderate). Framing the device as improving detection of the highest-risk CRC precursors is not supported by the pooled data.
- Which GRADE ratings to weight most heavily: High certainty for SSLDR and PDR; moderate for ADR (due to I²=64% heterogeneity) and for advanced ADR (due to imprecision). Clinicians and committees should treat the SSLDR and PDR findings as more reliable anchors for decision-making than the ADR estimate.
- COI and funding context: The anchor meta-analysis declared no industry funding and no author financial conflicts — a favorable profile relative to several of the individual included trials, particularly COLO-DETECT (Medtronic-funded). This does not eliminate all bias risk but reduces the most direct form of industry influence on pooled conclusions.
- Real-world applicability: Gains may be attenuated in high-ADR endoscopy units or when the system is used without complementary quality-improvement tools. Units with baseline ADRs at or above 45% should not expect the pooled RCT effect size to replicate without additional implementation support.
| Field | Detail |
|---|---|
| Primary Source | Sattar et al. (2025). Effectiveness of the GI Genius Computer-Aided Detection System Versus Standard Colonoscopy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cureus. |
| PMID / PMC | PMID 41246784 / PMC12616575 |
| Study Design | PRISMA-aligned systematic review and meta-analysis of 7 RCTs |
| Population | 9,639 patients across 7 RCTs (UK, France, Spain, Italy, US, multinational) |
| Primary Outcome | ADR: RR 1.12 (95% CI 1.03–1.22), I²=64%, GRADE moderate |
| Key Secondary Outcome | SSLDR: RR 1.27 (95% CI 1.11–1.47), I²=11%, GRADE high |
| Critical Null Finding | Advanced ADR: RR 1.01 (95% CI 0.90–1.13), p=0.85, GRADE moderate |
| Funding | No industry funding declared |
| Author COI | All authors declared no financial conflicts |
Comments
Join the discussion with an anonymous comment.